Recurrent IgE-Mediated Anaphylactic Transfusion Reactions with Normal IgA in a 98-Year-Old Woman: A Transfusion-Sparing Approach.
INTRODUCTION
Iron deficiency anemia (IDA) remains the most prevalent nutritional deficiency worldwide and a leading cause of morbidity in elderly patients with multiple comorbidities, in whom chronic blood loss, impaired absorption, and poor nutritional intake frequently coexist (1). While red blood cell (RBC) transfusion is a cornerstone of management in severe anemia, allergic transfusion reactions (ATRs) complicate up to 1–3% of all transfusions, with life-threatening anaphylaxis occurring in an estimated 1:20,000 to 1:50,000 RBC units representing one of the most feared non-hemolytic adverse events in transfusion medicine (2,3). Anaphylactic transfusion reactions are classically attributed to IgA or haptoglobin deficiency with corresponding antibodies; however, in many cases the underlying mechanism remains unidentified, posing a significant clinical challenge (2,4).
The present case is noteworthy for several reasons. First, it describes a 98-year-old morbidly obese woman with severe IDA (hemoglobin 59 g/L) and extensive comorbidities who developed two consecutive, severe IgE-mediated anaphylactic reactions to ABO-compatible packed RBCs despite normal serum IgA, ruling out the most commonly investigated etiology. Second, the case illustrates the diagnostic complexity of differentiating anaphylaxis from transfusion-related acute lung injury (TRALI), transfusion-associated circulatory overload (TACO), and acute hemolytic reactions in a hemodynamically fragile, multi-morbid elderly patient. Third, it demonstrates the successful application of a transfusion-sparing strategy using high-dose intravenous ferric carboxymaltose combined with an erythropoiesis-stimulating agent, achieving hemoglobin normalization within four weeks and obviating the need for further blood products (5).
The purpose of this report is to present the clinical course, diagnostic reasoning, and management of recurrent non–IgA-mediated anaphylactic transfusion reactions in a nonagenarian with severe IDA, and to highlight intravenous iron replacement with erythropoiesis-stimulating support as an effective, life-saving alternative when transfusion is contraindicated. This case underscores the need for heightened clinical vigilance, multidisciplinary coordination, and individualized transfusion planning in elderly patients with complex allergic profiles.
CASE PRESENTATION
Patient Demographics and Medical History
A 98-year-old morbidly obese female (body mass index 43 kg/m2) presented to the emergency department (ED) with a chief complaint of dry cough and high-grade fever of acute onset. Her medical history was extensive and is summarized in Table 1.
Table 1. Baseline Comorbidities and Clinical Background
Comorbidity | Relevant Details |
Type 2 diabetes mellitus | On treatment; random glucose 12.0 mmol/L on admission |
Hypertension | On antihypertensive therapy |
Dyslipidemia | On lipid-lowering therapy |
Hypothyroidism | Most recent TSH: 7 mIU/L |
HFpEF (GIDD) | EF >55%; impaired LV relaxation on echocardiography |
Chronic kidney disease, stage II | Baseline creatinine 108 µmol/L; eGFR 43 mL/min |
Morbid obesity | BMI 43 kg/m² |
Prior cholecystectomy | Gallbladder absent on imaging |
Chronic constipation | Poor dietary intake: raw milk and bread |
Family history | Positive for colon cancer |
The patient denied any prior history of blood transfusion, lower gastrointestinal bleeding, unintentional weight loss, or previous endoscopic evaluation. She reported chronic bony aches and a predominantly poor nutritional intake.
Initial Clinical Assessment
On examination, the patient was alert and oriented, not in distress, lying flat, and saturating well on room air with a Glasgow Coma Scale score of 15/15, fair judgment, and intact memory. Chest auscultation revealed equal bilateral air entry with no crackles or wheezes. Cardiovascular examination demonstrated normal first and second heart sounds with no added sounds. The abdomen was soft and lax. Lower extremities showed no swelling or pitting edema, with warm periphery and palpable peripheral pulses of good volume.
Initial Investigations and Diagnosis
Chest radiography revealed right middle lobe opacification with air bronchograms, consistent with community-acquired pneumonia (CAP). Respiratory multiplex polymerase chain reaction (PCR) was negative, including for Mycoplasma pneumoniae. Empirical antibiotic therapy with moxifloxacin was initiated.
Baseline laboratory investigations revealed a striking hematologic picture (Table 2). The patient’s hemoglobin two years prior had been approximately 100 g/L, indicating a progressive and significant decline.
Table 2. Admission Laboratory Investigations (25 August 2025)
Parameter | Result | Reference Range | Interpretation |
Hemoglobin | 59 g/L | 120–160 g/L | Severely low |
MCV | 54.3 fL | 80–100 fL | Microcytic |
MCH | 18.2 pg | 27–33 pg | Hypochromic |
MCHC | 335 g/L | 320–360 g/L | Normal |
RDW | 23.5% | 11.5–14.5% | Markedly elevated |
WBC | 20.00 × 10⁹/L | 4.0–11.0 × 10⁹/L | Leukocytosis |
Neutrophils | 86.3% | 40–70% | Neutrophilia |
Platelet count | 577 × 10⁹/L | 150–400 × 10⁹/L | Thrombocytosis |
Serum iron (Jan 2025) | 5.24 µmol/L | 10–30 µmol/L | Critically low |
Total IgE | 444 IU/mL | <100 IU/mL | Elevated |
Creatinine | 108 µmol/L | 50–100 µmol/L | Mildly elevated |
eGFR | 43 mL/min | >60 mL/min | Reduced |
Albumin | 27 g/L | 35–50 g/L | Low |
Sodium | 131 mmol/L | 136–145 mmol/L | Hyponatremia |
AST | 59 U/L | 10–40 U/L | Elevated |
LDH | Mildly elevated | 120–246 U/L | Mildly elevated |
IgA | Normal | Normal | Normal |
PT / INR | 12.50 s / 1.12 | 11–13.5 s / <1.2 | Normal |
Peripheral blood smear demonstrated moderate anisopoikilocytosis with occasional ovalocytes, elliptocytes, and polychromatic cells. White blood cells showed neutrophilia with a notable finding of hypersegmented neutrophils, raising the possibility of a concomitant megaloblastic process. Scattered reactive lymphocytes were observed. Platelets were increased with some large forms. No circulating blasts were identified. The hematology service was consulted and rendered an impression of severe iron deficiency anemia (IDA).
Anaphylactic Transfusion Reactions
Given the severity of the anemia (hemoglobin 59 g/L), a decision was made to initiate blood transfusion. One unit of unpooled packed red blood cells (UPRBC), blood type O-negative (matched to the patient’s O-negative blood type), was commenced at approximately 12:30 AM. The ensuing clinical course is outlined below:
First transfusion reaction: Within ten minutes of initiating the transfusion, the patient developed generalized pruritus followed by sudden-onset respiratory distress characterized by audible wheezing, progressing to hemodynamic instability with hypotension within 30 minutes. The transfusion was immediately discontinued. Intramuscular epinephrine (EpiPen) was administered with prompt and dramatic clinical improvement. A repeat chest radiograph showed persistent right middle lobe opacification. Post-reaction investigations revealed a positive direct antiglobulin (Coombs) test, mildly elevated lactate dehydrogenase (LDH), normal total bilirubin, and no increment in hemoglobin following the transfusion.
Second transfusion reaction: The following day, a second blood unit was administered, during which the patient developed a recurrent episode of anaphylaxis. This episode was more severe, necessitating two doses of intramuscular epinephrine for stabilization.
Table 3. Differential Diagnosis of the Transfusion Reaction
Diagnosis | Supporting Evidence | Against |
IgE-mediated anaphylaxis | Rapid onset (<30 min); dramatic response to epinephrine; elevated total IgE (444 IU/mL); recurrence with re-exposure | - |
TRALI | Respiratory distress; hypotension; temporal association | Dramatic response to epinephrine favors anaphylaxis; no bilateral infiltrates |
AHTR | Positive DAT; mildly elevated LDH | ABO-compatible (O–ve to O–ve); normal bilirubin |
TACO | Respiratory distress | Rapid onset; pruritus; hypotension (TACO causes hypertension); response to epinephrine |
IgA deficiency reaction | Anaphylaxis with transfusion | Serum IgA level was within normal limits |
A review of the patient’s medication history revealed prior receipt of intravenous ceftriaxone (one dose at an outside facility) and a seven-day course of amoxicillin–clavulanate in 2023. The absence of an immediate or delayed hypersensitivity reaction to ceftriaxone argued against beta-lactam allergy as a confounding etiology. The clinical presentation was ultimately most consistent with an IgE-mediated anaphylactic reaction to a component of the packed red blood cell unit.
Inpatient Management
Following the two anaphylactic episodes, a multidisciplinary approach was adopted. The hematology on-call team was emergently consulted on 23 August 2025. Discussion with the blood bank confirmed that an investigation into the cause of the reactions was ongoing. The consensus was that there was no immediate urgency for blood transfusion and that supportive measures should be prioritized. The management strategy is summarized below:
Table 4. Summary of Inpatient Management
Intervention | Details |
Iron replacement | IV ferric carboxymaltose 1,000 mg, followed by 500 mg one week later |
Erythropoiesis-stimulating agent | Darbepoetin alfa 40 U SC administered prior to discharge |
Additional investigations ordered | Vitamin B12, folic acid, methylmalonic acid, homocysteine, IgA, IgE levels |
Blood bank plan | SAGM-depleted pRBC authorized; to be given only in ICU if clinically indicated |
Transfusion precautions | Blood allergy flagged; no transfusion without contacting MRP; ICU setting mandatory |
Steroid therapy | Methylprednisolone and hydrocortisone administered; improving leukocytosis noted |
Antibiotic therapy (CAP) | Moxifloxacin continued |
Constipation management | Lactulose enema and glycerin suppositories (last BM 7 days prior) |
The hematology consultant evaluated the patient on 24 August 2025 and confirmed severe iron deficiency anemia with possible concomitant vitamin B12 or folate deficiency, suggested by the presence of hypersegmented neutrophils on blood smear. The team emphasized avoidance of blood transfusion wherever possible. Blood bank consultation confirmed that washed red blood cells were not available; however, saline-adenine-glucose-mannitol (SAGM)-depleted packed red blood cells could be provided if transfusion became clinically necessary.
Imaging Studies
A contrast-enhanced CT scan of the abdomen and pelvis was performed using a pancreatic mass protocol to evaluate for pancreatitis. No radiological evidence of pancreatitis was identified. The liver appeared dysmorphic with diffuse steatosis but no focal hepatic lesions or biliary dilatation. Portal and hepatic veins were patent. The gallbladder was absent, consistent with prior cholecystectomy. Bilateral simple renal cortical cysts and uncomplicated colonic diverticulosis were noted incidentally. The lower chest images confirmed right lower lobe consolidation with air bronchogram, consistent with pneumonia. No free fluid, lymphadenopathy, or suspicious osseous lesions were identified.
Transthoracic echocardiography (22 August 2025) demonstrated a technically difficult study with a poor acoustic window. The left ventricle was normal in size with preserved systolic function (ejection fraction >55%). Transmitral spectral Doppler flow pattern was suggestive of impaired left ventricular relaxation, consistent with grade I diastolic dysfunction. No regional wall motion abnormalities or pericardial effusion were noted. The right ventricle was normal in size and function.
Family Conference and Discharge
A family meeting was held with the patient and her son. The medical team proposed a trial of SAGM-depleted red blood cells under intensive care unit (ICU) monitoring to investigate the anaphylactic tendency and to establish a safe transfusion strategy for future needs. The family was counseled that declining the trial would result in discharge with weekly outpatient monitoring. Strict transfusion precautions were documented, including mandatory ICU administration and prior notification of the most responsible physician before any blood product administration.
By 26 August 2025, the patient’s hemoglobin had risen to 71 g/L, and she was clinically asymptomatic. She was discharged with a structured outpatient follow-up plan, including a subsequent IV iron infusion (500 mg) scheduled at the medical day unit, outpatient hematology follow-up, and review in the CTU clinic. Aspirin was withheld pending outpatient reassessment.
Outpatient Follow-Up and Response to Treatment
At follow-up on 18 September 2025, laboratory investigations revealed a dramatic hematologic recovery (Table 5). The response to IV iron and darbepoetin was robust, with hemoglobin more than doubling within four weeks.
Table 5. Comparison of Key Laboratory Parameters: Admission vs. Follow-Up
Parameter | Admission (25 Aug 2025) | Follow-Up (18 Sep 2025) | Trend |
Hemoglobin | 59 g/L | 122 g/L | ↑↑ Normalized |
MCV | 54.3 fL | 76.4 fL | ↑ Improving |
RDW | 23.5% | 36.0% | Dimorphic population |
WBC | 20.00 × 10⁹/L | 11.10 × 10⁹/L | ↓ Improving |
Platelet count | 577 × 10⁹/L | 386 × 10⁹/L | ↓ Normalized |
Serum iron | 5.68 µmol/L | 16.20 µmol/L | ↑ Improved |
TIBC | See note | 40.4 µmol/L | Low–normal |
UIBC | >89.5 µmol/L | 24.2 µmol/L | ↓ Normalized |
Vitamin B12 | N/A | 786 pmol/L | Normal |
Homocysteine | N/A | 7.9 µmol/L | Normal |
Methylmalonic acid | N/A | 229.10 nmol/L | Mildly elevated |
LDH | Mildly elevated | 191 U/L | Stable |
The elevated RDW of 36.0% at follow-up was consistent with a dimorphic red cell population, reflecting the concurrent presence of newly produced normocytic red cells alongside the residual microcytic population—a hallmark of hematologic recovery following iron replacement.
The hematology service reviewed the patient via virtual consultation on 25 September 2025 and concluded that the iron deficiency anemia had resolved. The patient was discharged from the hematology service with recommendations to avoid blood transfusion as much as possible and to pursue further investigation with gastroenterology and her primary care physician to identify the underlying etiology of the iron deficiency.
Gastrointestinal Evaluation
Given a positive fecal immunochemical test (FIT) and a strong family history of colon cancer, CT colonography was performed on 21 September 2025. The study was suboptimal as the patient refused carbon dioxide insufflation; intravenous and enteric contrast were administered as an alternative. No sizable colonic polyps or masses were identified. Extra-colonic findings were consistent with prior imaging and included diffuse hepatic steatosis, absent gallbladder, bilateral renal cortical cysts, and uncomplicated diverticulosis. Notably, the previously documented right lower lobe consolidation had resolved, confirming successful treatment of the pneumonia.
The gastroenterology service reviewed the CT colonography results with the family on 24 November 2025 during a virtual outpatient visit and provided reassurance regarding the absence of colonic malignancy. An allergy and immunology referral was placed for further evaluation of the transfusion-related anaphylaxis; however, contact could not be established with the patient at the time of the first scheduled virtual appointment on 24 November 2025.
DISCUSSION
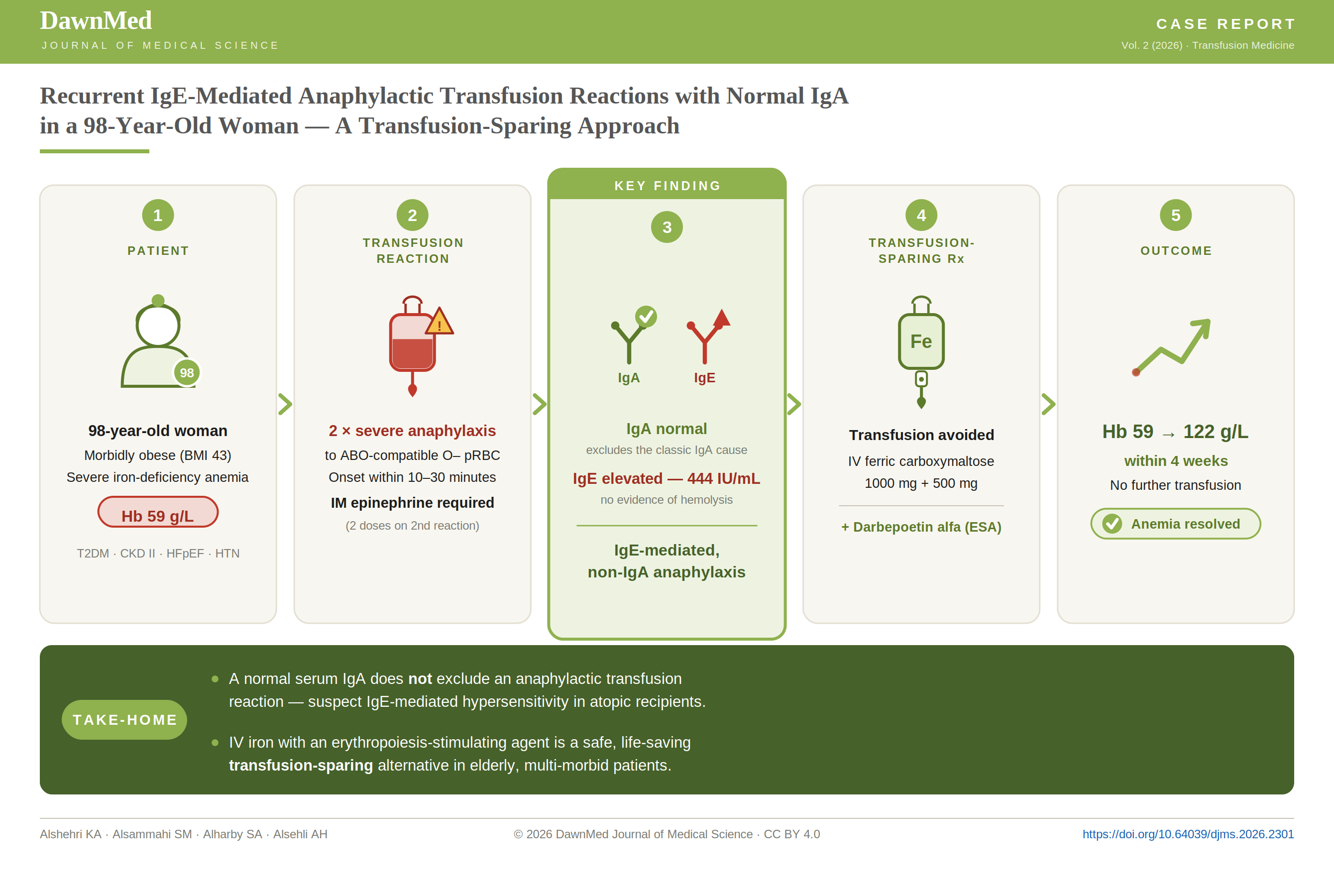
This report details a nonagenarian with severe iron deficiency anemia (IDA) and multiple comorbidities who developed two consecutive, severe anaphylactic reactions to ABO-compatible packed red blood cells (RBCs), occurring within 10–30 minutes of transfusion initiation and requiring repeated intramuscular epinephrine. Crucially, serum IgA was normal, a positive direct antiglobulin test was unaccompanied by biochemical hemolysis, and elevated total IgE (444 IU/mL) supported an IgE-mediated hypersensitivity mechanism. A transfusion-sparing strategy combining intravenous ferric carboxymaltose with darbepoetin alfa resulted in hemoglobin normalization (59 to 122 g/L) within four weeks, obviating the need for further blood products.
Anaphylactic transfusion reactions (ATRs) following RBC administration are rare, with hemovigilance data estimating severe reactions at approximately 7 per 100,000 transfusions, compared with 34 per 100,000 for all allergic reactions (3). Historically, IgA deficiency with anti-IgA antibodies was considered the prototypical cause; however, contemporary evidence has substantially challenged this paradigm. Sandler et al. demonstrated that fewer than 20% of suspected anaphylactic transfusion reactions are attributable to IgA deficiency, and subsequent hemovigilance analyses from France and the United Kingdom confirm that IgA-mediated reactions are exceptional rather than typical (6,7). This case aligns with the emerging consensus: an elderly recipient with entirely normal IgA levels developed recurrent severe anaphylaxis, reinforcing that clinicians should not rely solely on IgA testing to exclude or confirm an allergic etiology.
The pathogenesis of non-IgA-mediated ATRs is heterogeneous and incompletely understood. Recognized mechanisms include antibodies against haptoglobin (particularly in East Asian populations with Hp-deficiency), anti-Chido/Rodgers (anti-C4), passive transfer of donor-derived IgE or food allergens, and accumulation of biological response modifiers during component storage (2,8,9). Recipient atopic predisposition reflected by elevated total and allergen-specific IgE has been identified as a stronger predictor of ATRs than donor or product attributes (4,10). In the present case, the markedly elevated total IgE, rapid symptom onset, dramatic response to epinephrine, and recurrence on re-exposure strongly support an IgE-mediated, recipient-driven mechanism, possibly triggered by a plasma protein or passively transferred allergen in the donor unit. The positive direct antiglobulin test without hemolysis likely reflected a non-specific finding rather than an alloimmune process, consistent with the ABO-compatible transfusion.
Differentiating anaphylaxis from other acute transfusion reactions in a frail, multi-morbid patient is clinically demanding. Transfusion-related acute lung injury (TRALI), transfusion-associated circulatory overload (TACO), and acute hemolytic transfusion reactions can all present with respiratory distress and hemodynamic instability, yet their management diverges substantially. In this case, the absence of bilateral pulmonary infiltrates argued against TRALI; the presence of hypotension (rather than hypertension) and pruritus was inconsistent with TACO; and ABO compatibility with a normal bilirubin excluded significant intravascular hemolysis (4,11). The prompt and dramatic response to epinephrine—a therapy specific to anaphylaxis—was perhaps the most compelling clinical clue. Because no specific confirmatory test reliably identifies the causative allergen, diagnosis remains largely one of exclusion, supported by clinical pattern recognition and adjunctive testing for IgA, haptoglobin, and tryptase where available (6,11).
Acute management of transfusion-associated anaphylaxis mirrors that of anaphylaxis from any cause: immediate cessation of the transfusion, intramuscular epinephrine, airway support, intravenous fluids, and adjunctive antihistamines and corticosteroids (3,11). For patients requiring subsequent transfusion, evidence supports plasma reduction either through washing or concentrating cellular components as the most effective preventive measure. Tobian et al. demonstrated that washed RBCs reduced ATR incidence from 2.7% to 0.3%, an 89% relative reduction (12). Where washed products are unavailable, saline–adenine–glucose–mannitol (SAGM)-depleted RBCs represent a pragmatic alternative, as was planned for the present patient should transfusion become unavoidable. Critically, the decisive intervention in this case was avoidance of further transfusion through high-dose intravenous ferric carboxymaltose combined with an erythropoiesis-stimulating agent (ESA). This strategy has been shown to achieve transfusion independence in patients with chronic IDA and to safely correct anemia in elderly patients with multiple comorbidities who refuse or cannot tolerate RBC transfusion (5,13). Pre-medication with antihistamines or corticosteroids, while commonly practiced, has limited evidence for preventing recurrent severe reactions and should not substitute for definitive mitigation (10,11).
Several lessons emerge from this case. First, anaphylactic transfusion reactions can and do occur in IgA-replete patients; a normal IgA level does not rule out an allergic etiology and should not preclude rigorous transfusion precautions. Second, age and severity of anemia should not reflexively drive transfusion when an effective, non-transfusion pathway exists particularly in patients with demonstrated hypersensitivity. Third, a structured multidisciplinary response involving transfusion medicine, hematology, allergy/immunology, and critical care is essential for safe re-transfusion planning, including ICU-level monitoring, written transfusion precautions, and consideration of washed or SAGM-depleted products. Finally, correction of the underlying etiology of IDA, through investigation of gastrointestinal blood loss and nutritional deficits, must parallel acute anemia management to prevent recurrence.
Conclusion
This case demonstrates that a normal serum IgA does not exclude an anaphylactic transfusion reaction; in atopic recipients with elevated total IgE, an IgE-mediated mechanism should be actively considered and strict transfusion precautions maintained. In elderly, multi-morbid patients with severe iron deficiency anemia and demonstrated transfusion hypersensitivity, high-dose intravenous ferric carboxymaltose combined with an erythropoiesis-stimulating agent is a safe and effective transfusion-sparing alternative, achieving hemoglobin normalization within four weeks. Parallel investigation of the underlying cause of iron deficiency remains essential to prevent recurrence.
Declarations
Consent for publication: Written informed consent for publication of this case report and any accompanying clinical details was obtained from her legal representative.
Funding: The authors received no specific funding for this work.
Conflicts of interest: The authors declare no conflicts of interest.
Author contributions: All authors contributed to the conception, literature review, drafting, and critical revision of the manuscript. All authors have read and approved the final version.
Data availability: All data relevant to this case are contained within the article. Additional de-identified information is available from the corresponding author on reasonable request.