Necrotizing Pneumonia in a Young Female with Sickle Cell Disease: A Rare and Severe Complication
Introduction:
Necrotizing pneumonia (NP) is a rare but severe complication of bacterial pneumonia that involves aggressive bacterial invasion and an intense inflammatory response. Inflammation of lung tissue may lead to tissue destruction, and impaired blood supply to tissues may result in necrosis, liquefaction, cavitation, and abscess formation. [1] NP is most commonly caused by toxin-producing bacteria, such as Staphylococcus aureus (especially PVL-producing MRSA) [2], Streptococcus pneumoniae, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Escherichia coli. [3] Computed tomography (CT) is the diagnostic modality of choice, and chest radiography serves as an important initial imaging tool. Management typically begins with empirical broad-spectrum antibiotics, and if empyema is present, treatment should include antibiotic coverage for the anaerobes. Antibiotic selection should be guided according to the local resistance pattern. Surgical intervention should be considered if medical treatment fails or complications occur; interventions could include debridement, wedge resection, lobectomy, decortication, and pneumonectomy. [4] The objective of this case report is to describe a rare presentation of NP in a young female with SCD and to highlight the diagnostic challenges, management strategies, and clinical considerations associated with this uncommon but serious complication.
Case Presentation:
This case involves an 18-year-old female patient with a known case of SCD. She complained of right-sided chest pain radiating to the back, which was vaso-occlusive (VOC) in nature, with pain in the lower extremities. The patient had a history of splenomegaly since age 9 with frequent emergency room (ER) visits occurring every 3–4 months for VOC. She had experienced one episode of ACS with no previous central nervous system involvement. However, there was a history of severe pain episodes due to splenic sequestration and no joint pain. The patient was on folic acid but had declined hydroxyurea therapy despite counseling regarding its benefits.
She started to have abdominal pain with VOC, so she went to a medical complex hospital, was treated for 3 days, and was discharged.
After that her condition worsened; she developed a moderate-grade fever (38.1 °C) with shortness of breath, palpitations, and low oxygen saturation reaching 91% that required a nasal cannula. Imaging showed a right-sided pleural effusion, and she was diagnosed with ACS with pleural effusion. She was transferred to the intensive care unit for 3 days, where she was treated with 2 units of blood exchange and then maintained on IV fluids, analgesia, and enoxaparin, ertapenem, and levofloxacin. The patient was encouraged to use incentive spirometry and advised to maintain mobility as tolerated. She did not comply, however, but was discharged after clinical improvement.
Three weeks later, she came to the ER complaining of exertional dyspnea, a low-grade fever, tachypnea, shortness of breath, mild chest pain, tightness during deep breathing, and lower-limb pain despite the treatment she had received at the hospital. She also mentioned that she had lost about 7 kg within the last 2 weeks and that she had a positive family history for breast malignancy (in her mother).
She presented with an oxygen saturation of 96% on room air and a blood pressure of 108/40 mmHg, with a notably wide pulse pressure secondary to a low diastolic blood pressure.
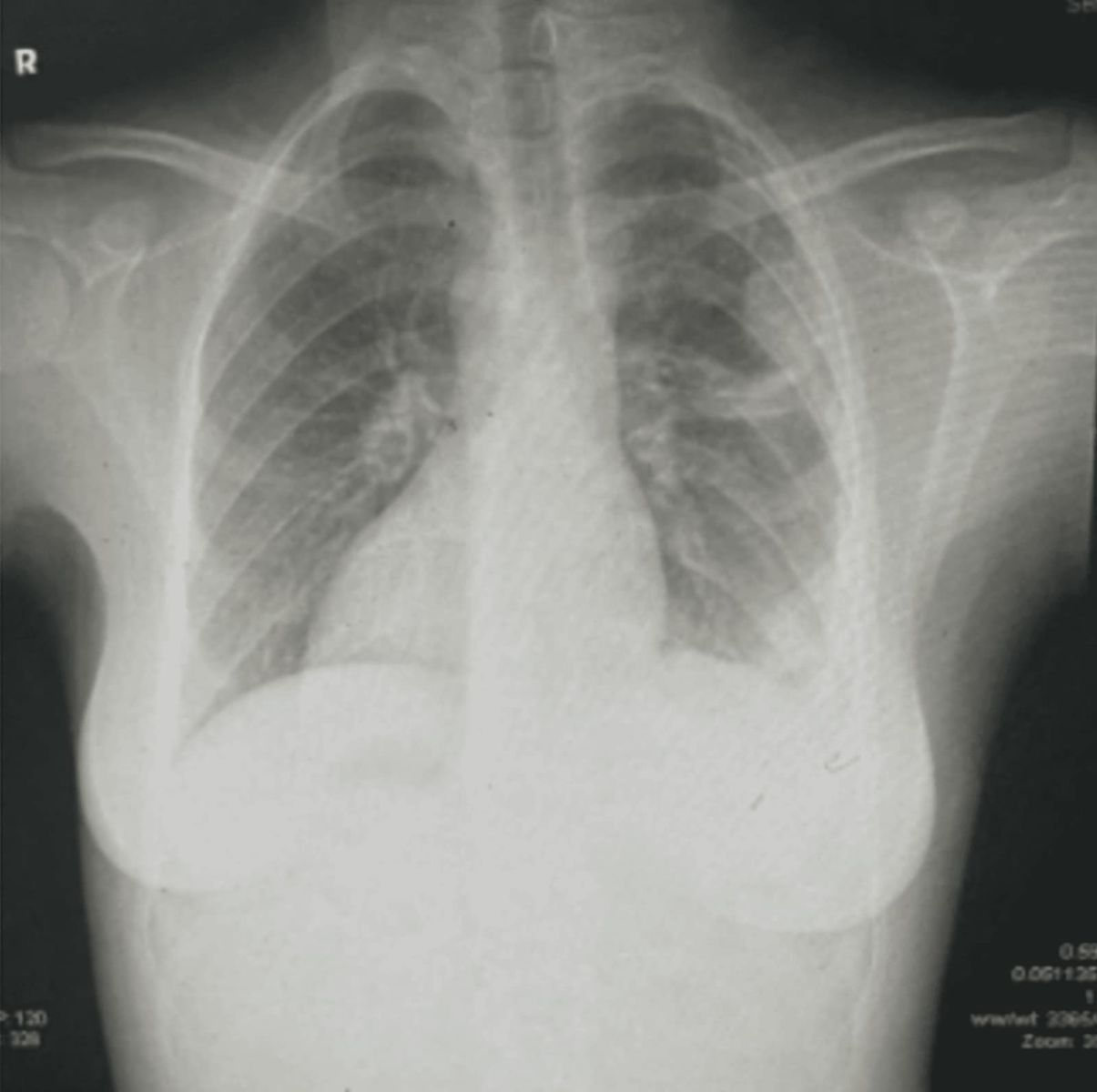
There were decreased breath sounds over the right lung field with hepatosplenomegaly. She was initially diagnosed as SCD with ACS. Labs were taken (Table 1) and showed no specific abnormality. Her ECG was unremarkable, and her chest X-ray showed non-resolving right-sided consolidation with loculated pleural effusion (Figure 1). Further testing was needed to rule out para-pneumonic effusion with empyema, hemothorax, or malignant pleural effusion. Hepatitis, HIV profile, and pleural fluid analyses were ordered and were unremarkable.
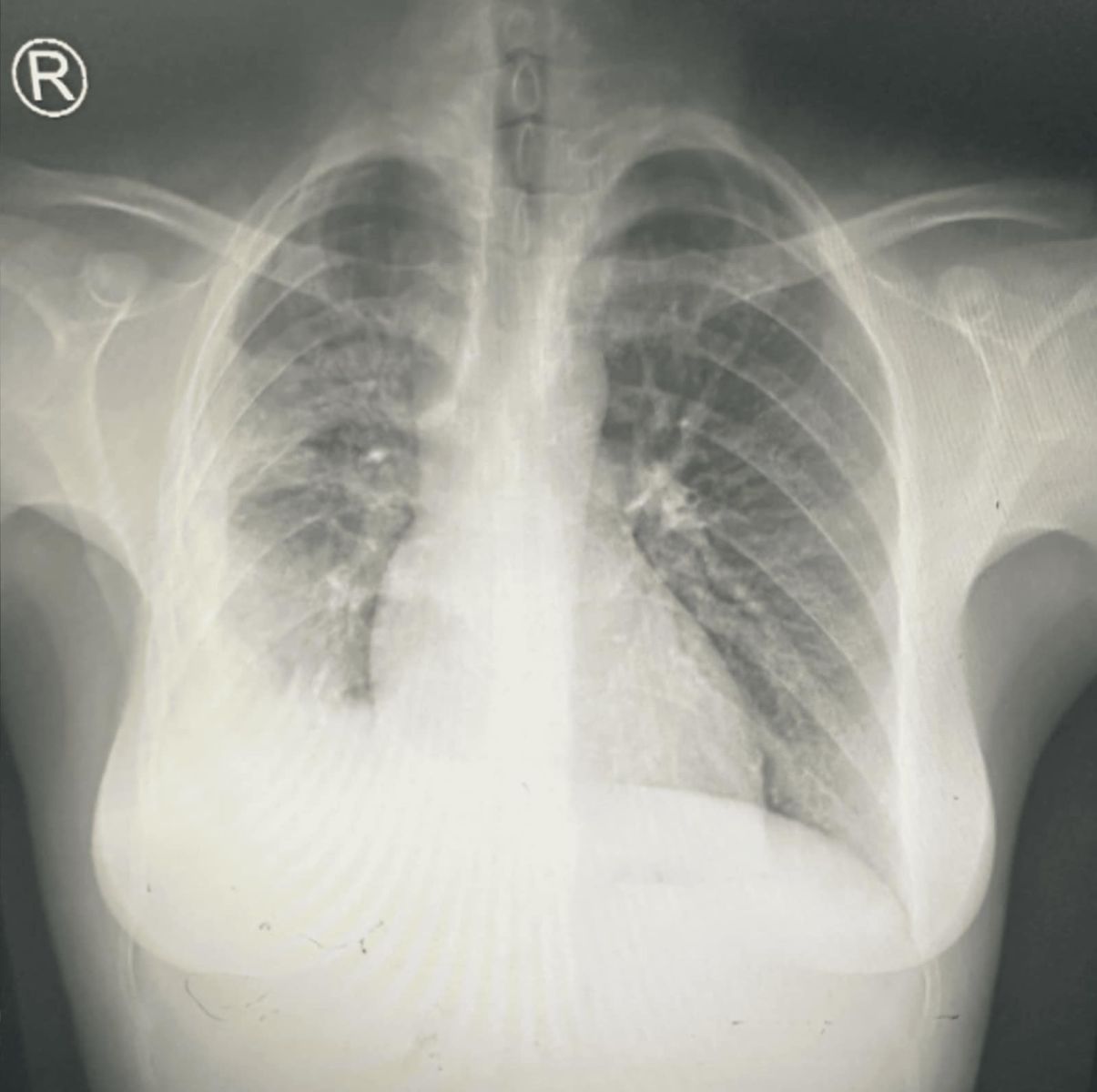
Figure 1: CXR showing non resolving right side consolidation with loculated pleural effusion
Laboratory Test | Actual Result | Normal Range |
WBC | 8.61 x 10^9/L | 4-10 x 10^9/L |
HGB | 9.92 g/dL | 12.1 – 15.1 g/dL |
Platelet | 797× 10⁹/L | 150,000 – 450,000 × 10⁹/L |
Reticulocyte Count | 1.26% | 0.5% – 2.5% |
Bilirubin (Total) | 28.42µmol/L | 1.7 – 20.5 µmol/L |
Bilirubin (Conjugated) | 13.06µmol/L | 0 – 5.1 µmol/L |
Creatinine | 55µmol/L | 44-97µmol/L |
LDH | 221U/L | 140 - 280 U/L |
Hepatitis | Negative | |
HIV profile | Negative | |
Table 1: labs in admission.
The laboratory findings demonstrate several notable features. The white blood cell count was within the normal range, which is somewhat unexpectedly normal in necrotizing pneumonia with empyema, and which is probably due to prior transfusion and antibiotic exposure from recent clinical interventions. The reticulocyte count was relatively low for a patient with sickle cell disease and is most likely attributable to recent transfusion therapy, which had suppressed endogenous erythropoietic activity. In addition, marked thrombocytosis was observed, likely reflecting a reactive inflammatory response in the setting of infection.
A CT showed a right-sided, small-sized pleural effusion associated with enhancement of the pleural reflection, which was highly suggestive of empyema. Right upper-lobe posterior-segment consolidative opacity with cavity-like structures reflected a lung abscess (Figure 2).
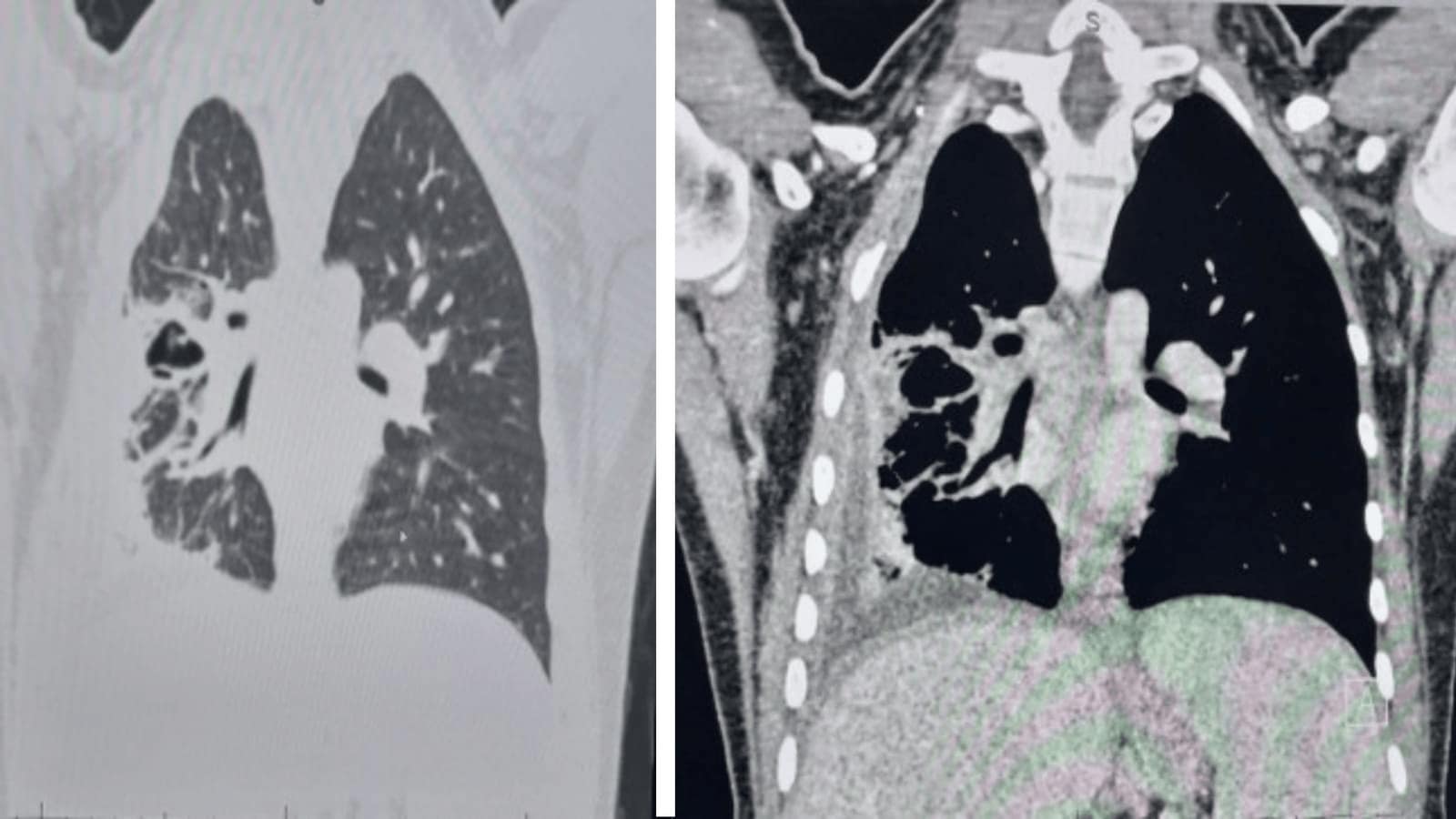
Figure 2: CT showed right-sided small-sized pleural effusion associated with enhancement of the pleural reflection
Bronchoscopy was performed, and bronchoalveolar lavage (BAL) samples were obtained from the affected lobe. A Gram stain, acid-fast bacilli (AFB) testing for tuberculosis, and methicillin-resistant Staphylococcus aureus (MRSA) cultures were all negative, with no significant microbial growth identified.
After multidisciplinary discussions involving the medical and surgical teams, it was confirmed that the patient had NP in the right lower and middle zones with a loculated collection suggestive of empyema. Because the patient was already on ertapenem and levofloxacin, after pulmonary consultation they suggested shifting it to piperacillin–tazobactam (Tazocin) 4.5 g IV for 7 days and then changing to amoxicillin–clavulanate (Augmentin).
Consultation to address the empyema, whether to perform drainage by chest tube or surgery, was conducted with thoracic surgery. The thoracic consultant advised pigtail insertion under ultrasound guidance. After the procedure was done, only 10 mL of pus was drained, so the pigtail was removed after 7 days. Then, after 5 days, video-assisted thoracoscopic surgery (VATS) and decortication were planned due to failure of conservative management.
According to the operative report documented by the surgical team, VATS demonstrated dense adhesions between the lung, chest wall, and diaphragm, with an associated abscess cavity.
After her condition improved, she was discharged on Augmentin and analgesia. Outpatient follow-up was planned with pulmonary, infectious disease, and thoracic surgery to check for improvement or any new complaints.
The patient was seen in the outpatient clinic by the thoracic surgeon after discharge. He mentioned that the wound was cleaned and the stitches were removed. Then she was seen by a pulmonary specialist, who advised her to continue on Augmentin and to do a contrast CT, which showed significant improvement (Figure 3).
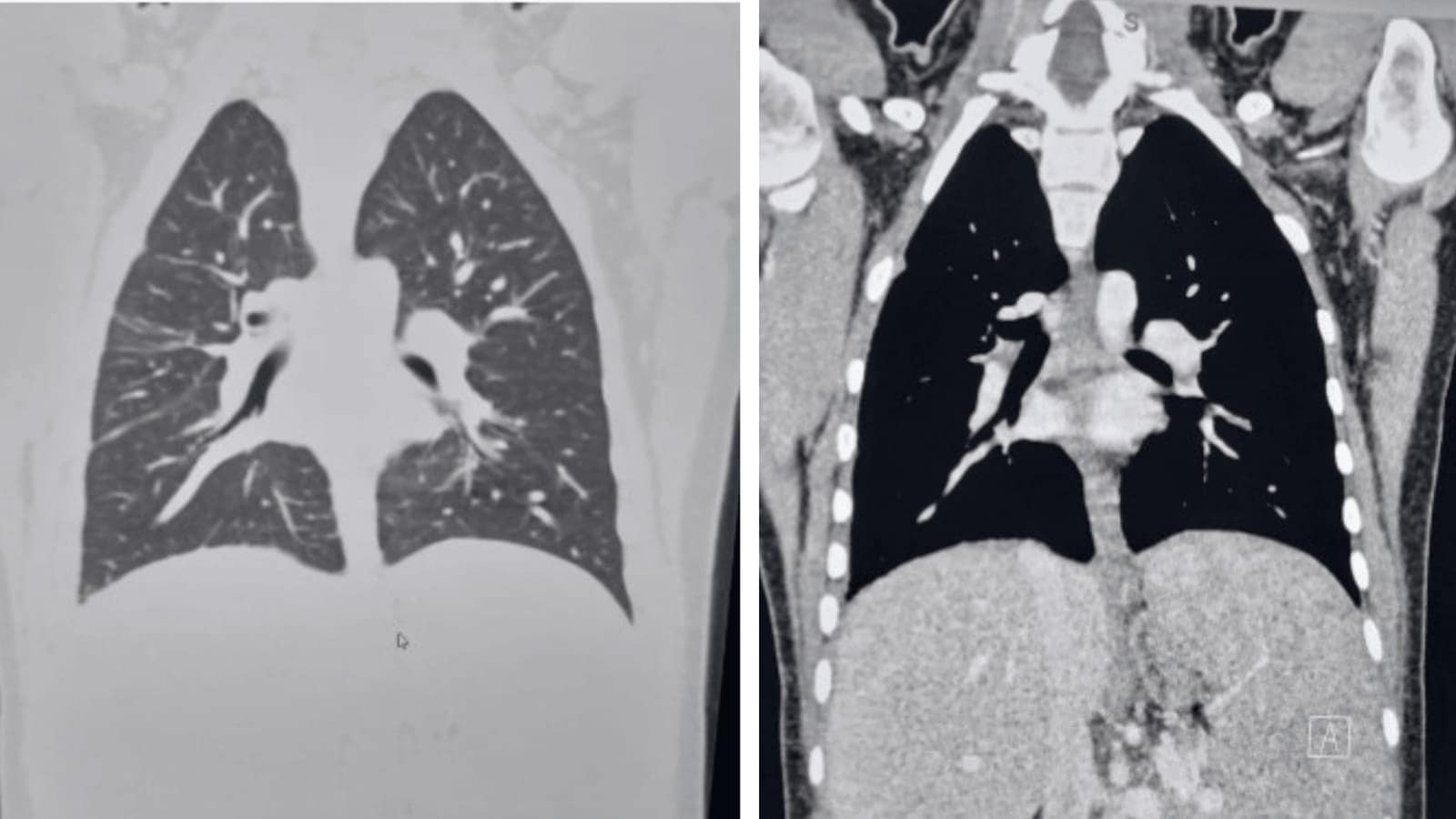
Figure 3: CT showing improvement after surgical and medical management
Her physician discussed with her the benefits of hydroxyurea, but she was not fully convinced. In addition, the Infectious disease agreed to continue on the same antibiotic, and X ray imaging was done (Figure 4).
Figure 4: Chest X-Ray confirming the improvement
Discussion:
Sickle cell disease (SCD) is a genetic disorder characterized by a defect in hemoglobin affecting the shape of red blood cells, leading to several presentations and complications, such as chronic hemolytic anemia, vaso-occlusion, and multiple infections, like pneumonia. The goal of disease-modifying therapy in SCD is to reduce the frequency of VOC and pain crises and to prevent long-term organ damage by increasing the presence of hemoglobin F. [5] In this case, the patient was not receiving hydroxyurea therapy due to treatment refusal despite prior counseling. However, cases of pneumonia resistant to treatment that lead to necrotizing pneumonia (NP) are unusual and rare in patients with SCD, particularly in young, fit individuals. [5] NP is a severe complication of mostly bacterial pneumonia, characterized by lung parenchymal destruction and cavitation. [6] NP can occur independently of acute chest syndrome (ACS), presenting unique diagnostic and management challenges. If not adequately treated, NP may lead to complications including bronchopleural fistula, empyema, respiratory failure, and septic shock. [4] Staphylococcus aureus is the most commonly implicated agent, followed by Streptococcus pneumoniae. [7] NP is uncommon, developing in only about 4–7% of community-acquired bacterial pneumonia, but incidents have increased of late, mostly seen in children, immunocompromised individuals, patients with chronic diseases like diabetes or chronic obstructive pulmonary disease (COPD), and patients with delayed or inadequate treatment of bacterial pneumonia, further complicating NP management. [4] NP is most commonly caused by toxin-producing bacteria, like Staphylococcus aureus (especially PVL-producing MRSA). [3,8] PVL-producing MRSA and methicillin-susceptible Staphylococcus aureus (MSSA) have been found to play significant roles in the development of NP. [9] Although no organism was isolated in our patient, S. aureus, particularly PVL-producing strains, is the most commonly reported cause of NP. [9,10]
PVL is a pore-forming toxin that, in animal studies, has been found to recruit neutrophils and cause inflammation, resulting in necrosis of lung tissue. [2] Identifying the definitive causative organism is usually challenging; we can get more accurate results from cultures of peripheral blood (if bacteremia is suspected), pleural fluid (if effusion is present), or infected lung tissue obtained during surgery. The overall positivity rate of microbiologic tests varies between 40% and 100%. [11] The definitive diagnosis is by chest CT, although chest radiography serves as an initial and highly valuable diagnostic tool for managing these patients.
Primary treatment usually starts with empirical broad-spectrum antibiotics, and if empyema is present, antibiotic coverage for the anaerobes should be added. Antibiotic selection should be guided according to the local resistance pattern. Surgical intervention should be considered if medical treatment fails or complications occur; interventions could include debridement, wedge resection, lobectomy, decortication, or pneumonectomy. [4,12]
Other case reports have illustrated the definition of NP; meanwhile, this case report discusses NP in a patient with SCD as well as the diagnosis, treatment, challenges, and prognosis according to the guidelines we were advised to use. However, if the patient shows no improvement even after aggressive medical therapy, there are no clear guidelines on when to start surgical treatment and intervention. NP may be a literature-based diagnosis, but in fact it might be undiagnosed or missed in unsuspected populations, especially as diagnosis requires imaging modalities rather than X-ray. Several clinical trials have assessed systemic corticosteroids for patients with severe community-acquired pneumonia. However, in patients with SCD, there is no evidence that they will help in treating NP; furthermore, they may worsen painful crises or lead to severe complications such as stroke. [13,14] Consequently, systemic corticosteroids were explicitly withheld from this patient’s management plan to avoid these significant risks. So, it is crucial to keep NP in mind when considering differential diagnoses for patients presenting with these symptoms, such as pulmonary embolism, ACS, and lung malignancy. Also, it is important to suspect NP, understanding that it can develop in SCD patients with severe or non-resolving pneumonia.
Furthermore, aggressive medical therapy has been shown to be beneficial as a practical approach along with timely surgical intervention for optimal outcomes, as shown in this case. Given this patient’s history of recurrent VOC, ACS, and splenic sequestration, continued counseling and hematology follow-up remain important components of long-term disease management.
Conclusion:
This case report remarks on the importance of early recognition of necrotizing pneumonia (NP) in sickle cell disease patients; NP can go undiagnosed due to its rare presentation and limited diagnostic tests and investigation. Thus, it is important to distinguish whether the condition is acute chest syndrome, NP, or a pulmonary embolism by using different investigation modalities. Furthermore, aggressive medical therapy has been shown to be beneficial as an effective approach along with timely surgical intervention for optimal outcomes, as shown in this patient.
Declarations
Conflicts of Interest: The authors declare that they have no conflicts of interest.
Funding: This research received no external funding..
Acknowledgements: None.
Author Contributions: All authors contributed equally to the conception, data collection, manuscript preparation, and revision of this case report. All authors reviewed and approved the final manuscript.
Patient Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Ethics Approval: Ethical approval was not required for this case report in accordance with institutional policies.
Data Availability: All relevant data are included within the article.