Awareness On the Benefits and Risks of Total Knee Replacement Among the Bisha Community
Introduction
The knee joint is the largest and most complex synovial joint, classified as a modified hinge joint. It consists of three main articulations: two between the femoral and tibial condyles, and one between the femur and the patella. Its primary movements are flexion and extension along a horizontal axis, though it also allows for a degree of rotational movement—referred to as locking and unlocking—around a vertical axis. Primarily responsible for bearing weight, the knee also plays a crucial role in movement. With human evolution leading to an upright posture, the lower limbs, including the knee joint, must support and balance the weight of the upper body. This constant load places the knee under continual stress, making it prone to wear and tear, which can disrupt its natural balance or homeostasis. Therefore, understanding the knee's normal anatomical structure and its functional limits is essential for anticipating and diagnosing potential joint disorders. [1] Alongside the knowledge of the knee physiology, kinematics and technology the incidence of total knee replacement is increasing. Total Knee Replacement (TKR), or knee arthroplasty, is considered to be a highly common orthopedic procedure and one of the cost-effective musculoskeletal surgical interventions worldwide; the number of patients undergoing this procedure is increasing. Painful knee osteoarthritis leading to reduced quality of life remains the main cause for total knee replacement. There is no defined threshold for this intervention, and it can be influenced by different factors that can be related either to the surgeon or to the patient himself. The majority of patients ended up with a satisfactory clinical outcome after this operation. [2]
Total knee arthroplasty is one of the successful and frequently performed procedures that improve knee function and relieve pain; in the 1970s and 1980s it became used worldwide and by now it is a highly effective intervention for patients with end-stage knee arthritis. Knee osteoarthritis is the most common indication for total knee replacement, as it improves function and relieves pain in patients with advanced osteoarthritis. [3] This intervention is effective as an option to treat chronic knee pain. Depending on the research and patient-based outcome measures, there was a considerable number of patients who experienced chronic knee pain, poor quality of life, functional disability and dissatisfaction after this intervention, and that was attributed mainly to the surgical technique and implant factors. In some cases the postoperative disability and pain cannot be medically explained. Many patient-related factors can contribute to the poor outcome of this procedure, including old age, female gender and low socioeconomic status, but those are not the only negatively affecting factors—psychological factors such as low social support, depression, somatization, low self-efficacy and poor pain-coping strategies also contribute. [4] To achieve a satisfying outcome from this intervention a proper examination, investigation and specific indication should be considered preoperatively. Osteoarthritis was the predominant cause for primary total knee replacement. [5] It is estimated that 4 million adults fifty years of age or older (4.2% of the population) currently are living with a total knee replacement; females with total knee replacement are more numerous than males, and the prevalence increases with age. [6]
Objectives
General objective: To determine the awareness of the benefits and risks of total knee replacement among the Bisha community.
Specific objectives:
- To assess the level of awareness regarding Total Knee Replacement (TKR) surgery within the Bisha community.
- To identify the perceived benefits and risks of TKR among patients in Bisha.
- To assess the awareness about factors influencing the decision to undergo TKR surgery within the community.
- To identify the sources of information about TKR that patients rely on in making decisions about the procedure.
Methods
This study utilized a cross-sectional design that was conducted in 2025 in Bisha city, which is located within the Aseer region in the southwestern part of Saudi Arabia. The study population was anyone from Bisha city, older than 18 years, male or female, who gave consent to participate.
Sample size calculation: N0 = Z²PQ/E²
- N0: the required sample size.
- Z: Z-value depending on the confidence level (1.96 for 95% confidence).
- P: estimated proportion of the population with the characteristic (approximately 50%).
- Q: complement of P (i.e., 1−P).
- E: margin of error, set at 5% (0.05).
The estimated sample size was 384; however, a larger sample of 441 respondents was adopted to improve reliability.
A convenience sampling technique was used, and data collection was done using an approved online-based questionnaire published through social media and WhatsApp to assess awareness among the surveyed sample of Bisha residents. The questionnaire was adapted from a validated tool previously used in orthopedic awareness studies to ensure relevance and validity. It covered key domains, including awareness of Total Knee Replacement (TKR) surgery, perceived benefits and risks of TKR, factors influencing the decision to undergo the procedure, sources of information about TKR, and cultural attitudes towards medical interventions. A pilot study was conducted involving 20 participants who were not included in the final analysis to test the clarity, reliability, and applicability of the questionnaire. Based on the pilot results, minor adjustments were made for improved comprehension. The questionnaire demonstrated acceptable internal consistency, with a Cronbach’s alpha value of 0.7, confirming its reliability for use in the main study.
Data were coded, entered, and analyzed using Statistical Product and Service Solutions (SPSS) (IBM SPSS Statistics for Windows, Version 27.0, Armonk, NY). Qualitative data were expressed in the form of numbers and percentages, and quantitative data in the form of mean and standard deviation. Data were presented in tables and graphs. The chi-square test was used for categorical variables between two groups of data. A p-value below 0.05 was considered statistically significant.
Results
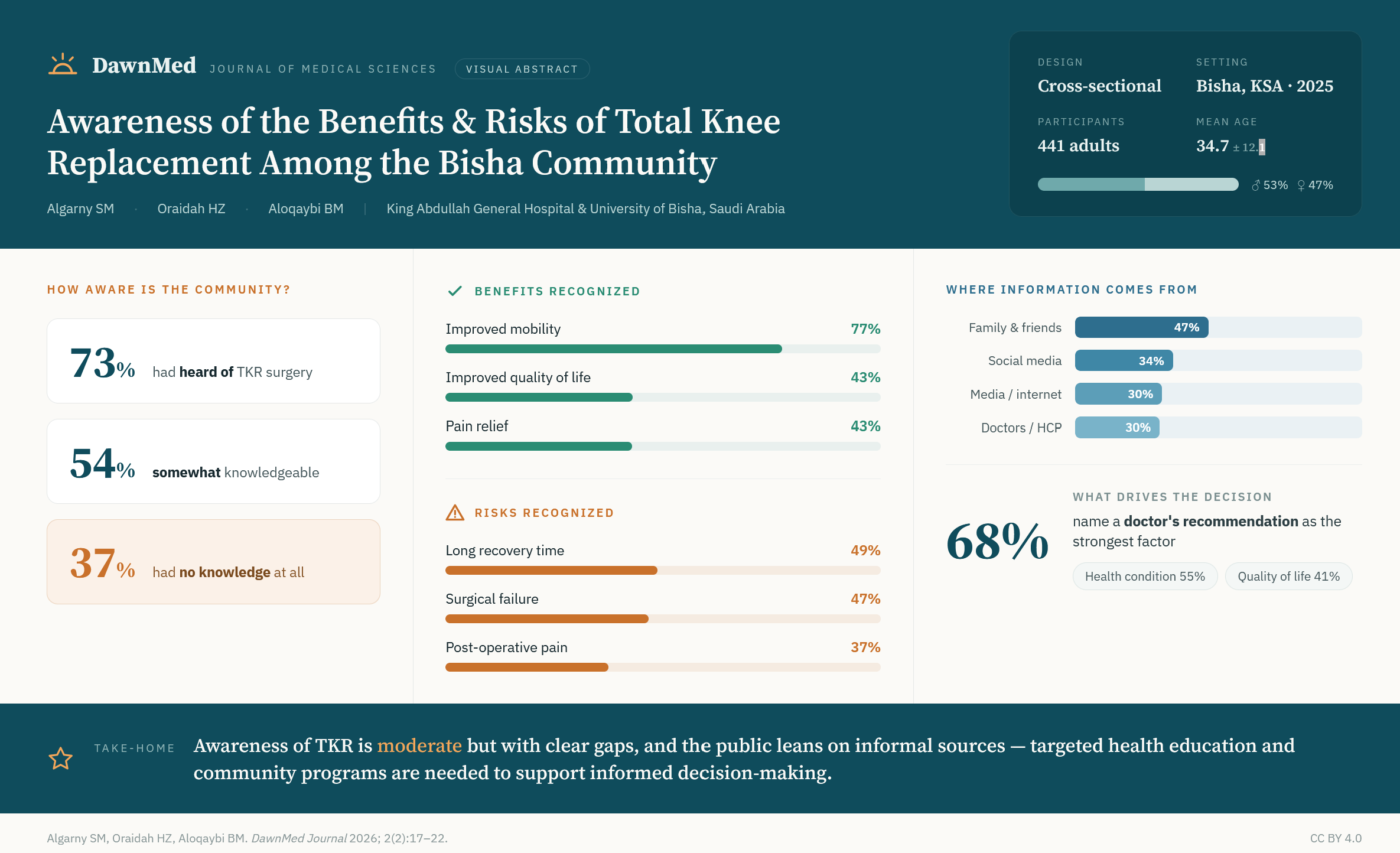
The total number of respondents who participated in the study was 441. Among these there were 206 females (46.7%) and 235 males (53.3%). The mean age and standard deviation of the respondents was 34.66 ± 12.142 years. With respect to occupation, those who were employed comprised the largest proportion 228 (51.7%), followed by students 111 (25.2%). Housewives accounted for 45 (10.2%) while the unemployed were 32 (7.3%). A small proportion comprised the retired 13 (2.9%) followed by those in other occupations 12 (2.7%). As for education level, most of the respondents had attained higher education 333 (75.5%) followed by those who had secondary education 96 (21.8%) (Table 1).
Table 1. Demographic characteristics of the respondents.
Variable | Category | n (%) |
Age (years), mean ± SD | — | 34.66 ± 12.142 |
Sex | Female | 206 (46.7) |
| Male | 235 (53.3) |
Occupation | Student | 111 (25.2) |
| Employed | 228 (51.7) |
| Retired | 13 (2.9) |
| Housewife | 45 (10.2) |
| Unemployed | 32 (7.3) |
| Other | 12 (2.7) |
Education level | Higher education | 333 (75.5) |
| Secondary | 96 (21.8) |
| Middle | 7 (1.6) |
| Primary | 5 (1.1) |
Figure 1 represents the proportion of respondents who were familiar with the total knee replacement surgery procedure. The majority of respondents 320 (73%) cited familiarity with the procedure, while a small percentage 121 (27%) were not familiar.
Figure 1. Proportion of respondents who have heard about TKR surgery (N = 441).
Table 2 summarizes participants’ awareness, perceived benefits, and perceived risks regarding Total Knee Replacement (TKR) surgery. The majority of respondents were somewhat knowledgeable about TKR (240, 54.4%), although a notable proportion (163, 37.0%) reported having no knowledge at all. When asked about conditions treated by TKR, the most commonly cited were knee joint deterioration (286, 64.6%), knee injuries (198, 44.9%), and arthritis (154, 34.9%), indicating a fair understanding of its primary indications. Regarding perceived benefits, improved mobility was the most recognized benefit (341, 77.3%), followed by improved quality of life (190, 43.0%) and pain relief (189, 42.9%). In terms of perceived risks, participants most frequently identified a long recovery time (215, 48.8%), surgical failure (206, 46.7%), and post-operative pain (165, 37.4%). Other notable concerns included nerve and blood vessel injury (160, 36.3%) and blood clots (141, 31.9%), highlighting an awareness of common post-surgical complications.
Table 2. Awareness, benefits and risks of TKR.
Research item | Category | n (%) |
How would you describe your knowledge of total knee replacement surgery? | I have no knowledge at all | 163 (37.0) |
| Knowledgeable of the word | 38 (8.6) |
| Somewhat knowledgeable | 240 (54.4) |
What conditions do you believe TKR surgery is used to treat? | Arthritis | 154 (34.9) |
| Knee injuries | 198 (44.9) |
| Knee joint deterioration | 286 (64.6) |
| Osteoporosis | 62 (14.0) |
| Knee joint instability | 128 (29.0) |
| Failure of conservative treatment | 103 (23.4) |
| Other | 7 (1.6) |
In your opinion, what are the main benefits of undergoing TKR surgery? | Pain relief | 189 (42.9) |
| Improved mobility | 341 (77.3) |
| Prevention of further joint deterioration | 160 (36.3) |
| Restoration of joint strength | 163 (36.9) |
| Improved quality of life | 190 (43.0) |
| Treatment of joint deformity | 81 (18.4) |
What are the main risks associated with TKR surgery? | Infection | 70 (15.9) |
| Blood clots | 141 (31.9) |
| Pain | 165 (37.4) |
| Surgical failure | 206 (46.7) |
| Long recovery time after the operation | 215 (48.8) |
| Nerve and blood vessel injury | 160 (36.3) |
| Other | 4 (0.9) |
Figure 2 presents the respondents’ sources of information on TKR surgery. It was revealed that most of the respondents got their information from family and friends 205 (46.5%) followed by those who heard it from social media 151 (34.2%). Those who got information from media (TV, radio, internet) were 134 (30.4%) while those who got information from doctors or healthcare professionals were 130 (29.5%). A small proportion got their information from community healthcare programs 71 (16.09%).
Figure 2. Respondents’ sources of information on TKR surgery.
Figure 3 illustrates the respondents’ interest in attending an awareness seminar about TKR surgery. Most of the respondents 186 (42%) said “maybe,” 178 (40%) expressed interest, while 77 (18%) were not interested.
Figure 3. Respondents’ interest in attending an awareness seminar about total knee replacement.
Figure 4 illustrates the factors influencing decision-making on TKR surgery. Regarding the decision to undergo TKR surgery, the majority of respondents pointed out that a doctor’s recommendation 300 (68.0%) would be their greatest influencing factor. Those who would be influenced by their health condition comprised 241 (54.6%), followed by the potential for improved quality of life 180 (40.8%). Those who could be influenced by the opinion of family and friends constituted the smallest proportion 63 (14.3%).
Figure 4. Factors influencing decision-making on TKR surgery.
Table 3 shows no statistically significant association between socio-demographic factors and knowledge scores regarding TKR awareness, benefits, and risks. Although males and those with higher education had slightly better knowledge, the differences were not significant (gender p = 0.749, occupation p = 0.318, education level p = 0.521). Notably, students and participants with higher education showed a trend toward higher knowledge levels.
Table 3. Relationship between socio-demographic variables and respondents’ knowledge score on awareness, benefits and risks of TKR.
Variable | Category | Poor | Average | Good | P value |
Gender | Female | 66 (47.8) | 64 (44.1) | 76 (48.1) | 0.749 |
| Male | 72 (52.2) | 81 (55.9) | 82 (51.9) | |
Occupation | Student | 23 (16.7) | 38 (26.2) | 50 (31.6) | 0.318 |
| Employed | 77 (55.8) | 78 (53.8) | 73 (46.2) | |
| Retired | 3 (2.2) | 5 (3.4) | 5 (3.2) | |
| Housewife | 18 (13.0) | 10 (6.9) | 17 (10.8) | |
| Unemployed | 13 (9.4) | 11 (7.6) | 8 (5.1) | |
| Other | 4 (2.9) | 3 (2.1) | 5 (3.1) | |
Education level | Higher education | 99 (71.7) | 108 (74.5) | 126 (79.7) | 0.521 |
| Middle | 2 (1.4) | 4 (2.8) | 1 (0.6) | |
| Primary | 1 (0.7) | 2 (1.4) | 2 (1.3) | |
| Secondary | 36 (26.1) | 31 (21.4) | 29 (18.4) | |
Data are presented as frequencies (n) and proportion (%). Knowledge-score categories are Poor / Average / Good. Pearson’s chi-square test was used to determine statistical significance; p < 0.05 was considered significant.
Discussion
Knee osteoarthritis is a progressive degeneration of articular cartilage that impacts quality of life. Total Knee Replacement (TKR) is an elective procedure aimed at relieving pain and restoring function. [7,8] Knee osteoarthritis remains one of the most common conditions in primary care. [9] Our study aimed at assessing the awareness of the benefits and risks of total knee replacement specifically among the Bisha community and found 54.4% of respondents reporting being somewhat knowledgeable, while 37% admitted to having no knowledge at all. This is in line with global trends, where limited public awareness about TKR has been reported in multiple studies. The findings on the low level of awareness are, for instance, supported by a study carried out in Saudi Arabia that revealed that while knee osteoarthritis was prevalent, many patients lacked adequate knowledge about surgical treatment options, often delaying intervention due to misinformation or lack of awareness. [10] Similarly, another study done in Hong Kong highlighted that while many patients had heard of joint replacement surgery, their level of understanding of the procedure, benefits, and risks was incomplete, and was largely shaped by non-medical sources. [11]
Our study also found that the majority of respondents associated TKR with improved mobility (77.3%), followed by improved quality of life (43.0%) and pain relief (42.9%). These perceptions align with clinical evidence from a study analysis that revealed TKR significantly enhances functional mobility and reduces chronic pain in patients with severe knee osteoarthritis. [12] However, some benefits such as restoration of joint strength (36.9%) and prevention of further joint deterioration (36.3%) were less recognized, indicating potential gaps in patient education regarding the full scope of surgical outcomes.
Our study results further revealed that respondents demonstrated awareness of some postoperative risks, such as long recovery time (48.8%) and surgical failure (46.7%); fewer recognized infections (15.9%) and blood clots (31.9%) despite these being among the most serious postoperative complications that can significantly impact recovery and patient outcomes. This is concerning, as infection and venous thromboembolism are major risks following knee replacement surgery.
Regarding sources of information, the study found that a majority of participants relied primarily on family and friends (46.5%) and social media (34.2%), while only 29.5% obtained information directly from healthcare professionals. This underscores the role of informal sources and networks in shaping public perceptions. This is alarming, as misinformation from non-medical sources may contribute to misconceptions about total knee replacement surgery. Similar findings were reported in a study in India, where a significant proportion of the population obtained health-related information from informal sources, leading to delays in seeking appropriate medical interventions. [13] The relatively low percentage of respondents receiving information from community health programs (16.09%) suggests a gap in structured public education efforts, which could be addressed through targeted community outreach initiatives.
The analysis revealed no statistically significant association between gender, education level, or occupation and knowledge scores about TKR (p > 0.05), suggesting that awareness deficits are widespread across all segments of the community rather than concentrated within specific demographic groups. This finding contrasts with a study by Almaawi et al., which reported a significant association between gender and awareness, but no significant link with education level. [14] Although not statistically significant, a trend was observed in which individuals with higher education exhibited better knowledge scores, with 79.7% demonstrating good knowledge. This aligns with evidence from other studies suggesting that higher education is associated with improved health literacy and a greater tendency to seek accurate medical information. [15] Additionally, an encouraging trend was noted among students, whose knowledge improved from 16.7% classified as poor to 31.6% as good, implying that younger and more educated individuals may be more receptive to health education initiatives.
Limitations
Given that the study relied on self-reported online survey data, recall bias and social desirability bias may have affected its accuracy and reliability. Furthermore, convenience sampling through WhatsApp and social media over-represented younger, more educated residents (75.5% with higher education), limiting generalizability to older and less digitally connected groups and to other populations.
Conclusion
The study reveals the presence of moderate awareness of TKR surgery among the surveyed sample of the Bisha community. While improved mobility and pain relief were commonly recognized benefits, serious postoperative risks such as infection and blood clots were less well acknowledged. There are significant knowledge gaps regarding its benefits, risks, and indications. The reliance on informal sources of information such as family and friends, and the underestimation of critical risks such as infection and blood clots, suggest an urgent need for structured programs aimed at educating the public. Given that a doctor’s recommendation plays a pivotal role in decision-making, healthcare providers should prioritize conducting preoperative counseling.
Recommendation
To increase the awareness of the population about total knee replacement, community-based health programs, digital media campaigns, and hospital-led patient education initiatives should be carried out to enhance public understanding and encourage timely surgical interventions.
Declarations
Conflict of Interest: The authors declare that there is no conflict of interest regarding the publication of this article.
Funding: None.
Authors’ Contributions: All authors contributed equally to all processes of the research work. They have read and agreed to the published version of the manuscript.
Ethical Approval and Informed Consent: Ethical approval was obtained from the Ethics and Research Committee of the College of Medicine, University of Bisha (Ref No: UB-RELOC H-06-BH-087/(02/04/46)). There was strict adherence to ethical principles such as confidentiality, anonymity, and informed consent. All participants provided consent before participating in the study questionnaire, and those who did not consent were immediately excluded before starting the questionnaire.